What is Family Medicine?
Family Medicine is a discipline and art of medical practice that gives balanced attention to the patient’s biomedical problems and the contextual problems of the patient and family experiencing the illness. Biomedical problems relate to the patient’s physical issues concerning the disease. Patient context problems relate to four pillars, which are described as follows:
Comprehensive and Continuous
The principle is that all diseases, especially catastrophic ones, are a long continuum starting from: healthy – at risk – pre-disease – definitive disease established – early complication – late complication – dying.
An example of disease progression is a long journey, such as in diabetes, which starts with genetic risk from the family, lack of physical activity, unbalanced diet, and non-adaptive stress management. If diabetes is already present and not managed properly, the disease will continue on a deteriorating path, starting from diabetic neuropathy, diabetic gangrene, diabetic nephropathy, and various other complications.
A doctor with a family medicine perspective will be aware of every stage of the disease progression and take appropriate and adequate health measures to reverse the direction for the better, or, if in the advanced stage, strive to improve the quality of life and emphasize a spiritual approach for the patient as preparation for the end of life, and also for their family, thereby reducing the negative health impact following the loss of a family member.
Doctors who graduate from FK UMS with a family medicine perspective are not only capable of establishing a diagnosis and managing the disease according to lege artis (standard medical procedure), but are also aware of current clinical problems and future problems related to the continuum of care, and are capable of taking appropriate and adequate action to optimally manage the disease.
Holistic
The holistic understanding guides the doctor to conduct examinations and management not only focusing on the biomedical aspect but also on the psycho-social aspects. Understanding the physical aspect of the disease, from pathophysiology to clinical manifestations, is the biomedical perspective.
The patient’s psychological aspect can be understood, especially in catastrophic diseases, as illustrated by the following example:
A patient is diagnosed by their family doctor with type two diabetes. The attending doctor has explained the disease at length. When asked by her child at home, the patient replies, “Mom is not sick, she is healthy.” This statement by the mother with diabetes to her child is an example of “denial” in the patient’s psychological acceptance of her illness.
There are five stages/types of a patient’s psychological acceptance of their suffering: denial, anger, bargaining, depressed, and accepted.
Denial. Denial or rejection in the form of a verbal statement, as in the example above, or the attitude of seeking alternative medicine to soothe their psychological state, is certainly not favorable in further disease management efforts.
Anger. Anger is a psychological phenomenon when a person experiences something contrary to their deepest hope. This anger can be directed at oneself, other family members, or even God. This anger is also not favorable in further disease management efforts.
Bargaining. Bargaining means a form of negotiation; some patients who are “already” sick and feel miserable because of it make a kind of “bargain” with God. “God, if I am cured, I will never yell at my wife again,” and so on. For those who are Muslim, they might make a vow (nadzar), “if I recover, I will…,” and so on.
Depressed. Some patients, after being diagnosed with a disease and enduring discomfort for so long, experience a period filled with feelings of emptiness; sadness permeates their lives on a deeper level. At this stage, some patients question, “why should I take medicine, it has no effect on me.”
Acceptance. In the Muslim community, acceptance is characterized by patience in facing the suffering of the illness, or at an even higher level, ridho (sincere contentment), enjoying the suffering because it comes from Allah SWT. Furthermore, there is a sense of responsibility to follow and engage with the health program jointly planned with the doctor.
The duty of a doctor with a family medicine perspective is to educate and persuade the patient so that their acceptance of the illness is in the acceptance phase.
Patient-Centered
In cases of illness, especially catastrophic diseases, every patient generally has a deepest desire, but that desire is hindered by the disease they are suffering from. Patient-centered medical service assures the patient that the medical intervention program undertaken is a collaborative effort by the doctor, patient, and family to achieve the patient’s deepest desire that is hindered by the illness.
Case illustration: In osteoarthritis, a grandfather has a deepest desire to be able to take his beloved grandchild to soccer lessons. However, this deepest desire is hindered by the osteoarthritis he suffers from. A patient-centered medical program focuses on this deepest desire, namely, “enabling the patient to take his grandchild to soccer lessons, through a program of weight loss, a balanced diet, and relevant physical activity.” The basic question for a family medicine doctor to the patient is, “What is your deepest desire while experiencing this illness?”
Patient-centered medical service also considers what is familiar to the patient, such as local customs or culture in the patient’s context, beliefs, and aspects of the patient’s spirituality/religiosity.
Family Approach
Functionally, within a family, there are three main roles generally played by the head of the family (husband/father) and the mother/wife. These three roles include the breadwinner, caregiver, and decision-maker. These three roles are important in family health management. The technical individual management of a patient within the family requires another family member to act as the caregiver, a role generally fulfilled by the mother/wife.
The role of the breadwinner and the decision-maker are crucial in providing financial support and in selecting the health facility or the type of assistance to be sought for the care of the sick family member. The caregiver’s role can be extended beyond when a family member is sick; in their capacity as the primary partner in implementing curative actions, they should also be involved in participating as a partner in implementing health promotion and prevention
Strategy for the integration of Family Medicine into the FK UMS curriculum
One of the characteristics of the competency-based curriculum in medical education is the presence of the SPICES approach, which is an acronym for Student-centered, Problem-based, Integrated, Community (and family) oriented, Early Clinical (community and family) exposure, and Systematic.
Student-centered is a learning strategy that positions students as active, responsible adults in the learning process.
Problem-based is a learning strategy that provides clinical/community problem scenarios as triggers for learning, motivating students to acquire learning outcomes. With these problem triggers, students gather information from various trusted scientific sources as learning material.
Integrated is a learning strategy that integrates various disciplines both vertically and horizontally, allowing students to integrate various learning outcomes that are highly useful for forming clinical reasoning in solving the professional problems they face.
Community and family oriented is a learning strategy oriented towards the needs of the community or families whose members experience health problems at various stages of the disease progression. Student learning is not limited to the classroom but also involves confronting and learning how to identify problems and determine solutions within the community.
Early Clinical, community, and family exposure is a learning strategy that exposes students early on to real-world clinical, community, and family settings. This strategy is realized through school- and fostered-village-based learning activities. Starting from the second semester, students are given learning experiences to apply clinical skills, communication, and individual approaches in real-world settings.
Systematic is a learning process structured systematically, logically, and in terms of material and competencies, ensuring that students acquire a more complex understanding, skills, and competencies as established in the graduate learning outcomes.
The integration of family medicine into the FK UMS curriculum is carried out gradually, sequentially, and involves early exposure of students to family, community, and clinical settings.
The integration of family medicine in undergraduate medical education is implemented through:
Family medicine block lectures integrated into every relevant block theme.
Tutorials that integrate learning objectives into every scenario-based learning session.
Field labs held once every semester, starting from the 2nd semester until the 7th semester, either independently or with an interprofessional education approach.
The dedicated Family Medicine Block.
The integration of family medicine in medical professional (clinical/clerkship) education is implemented through:
Family education assignments for patients cared for in every clinical rotation passed.
Family Medicine rotation as one of the required clinical learning rotations.
Field Lab Faculty of Medicine Universitas Muhammadiyah Surakarta
Field Lab as a strategy for achieving the competency of Family Medicine Excellence at FK UMS
Field lab is a field learning activity where students are given the opportunity to apply some of the competencies they have acquired from the learning carried out in block lectures, laboratory practicums, and related clinical and community skills. The Field Lab topic follows the selected block in the corresponding semester.
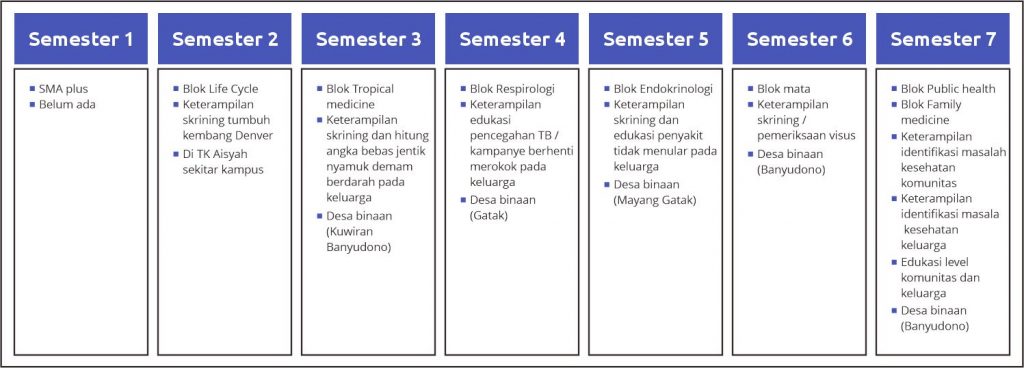
The Field Lab activities organized at FK UMS are scheduled every semester, corresponding to the selected block. The matrix of Field Lab topics, selected blocks, and semester placement is presented in figure 1. The following matrix shows the distribution of skills, selected blocks, and community/family application,
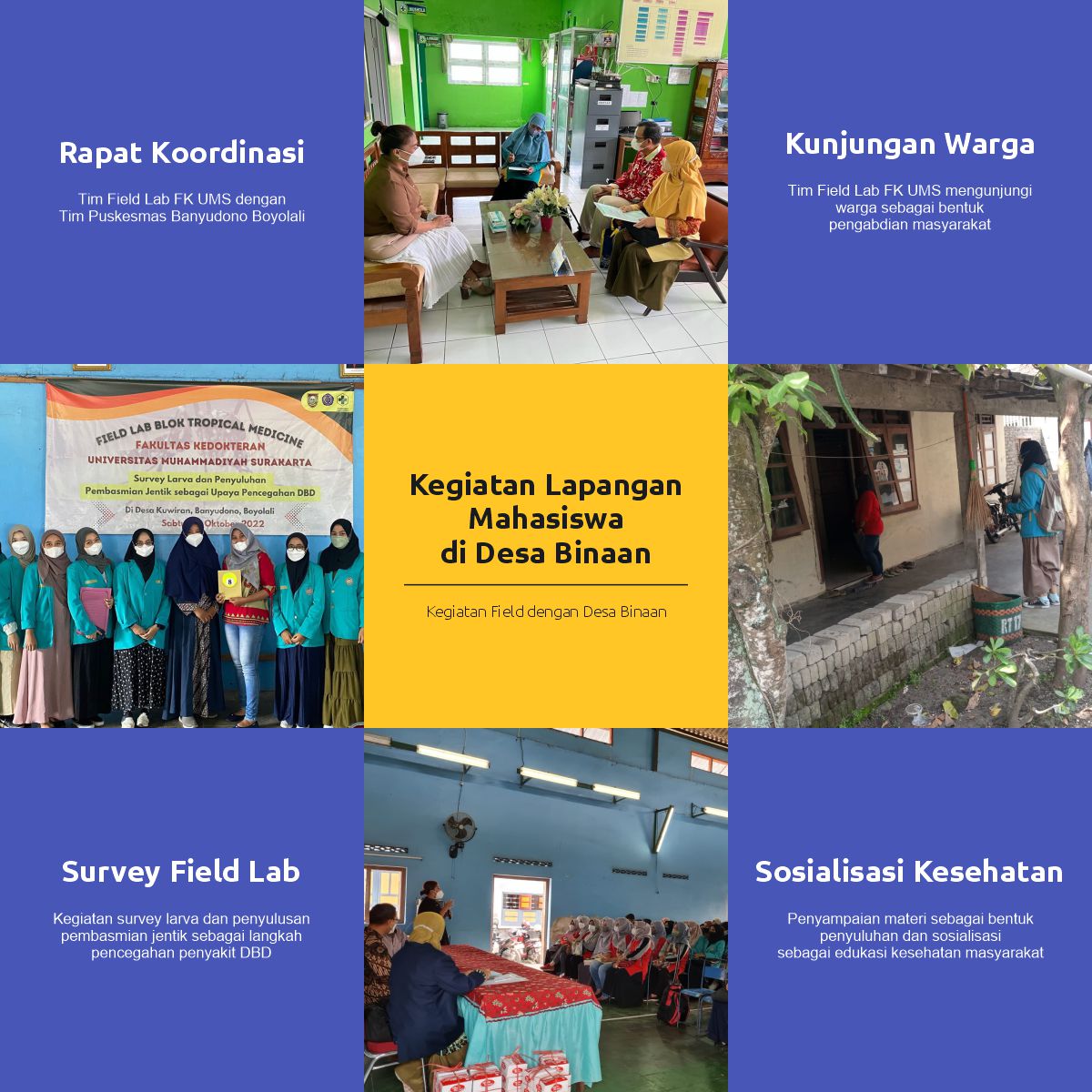
Activities of the Field Lab at the Faculty of Medicine, Universitas Muhammadiyah Surakarta
The elements involved in Field Lab activities are: students, campus supervising lecturers, field mentors, and the head of the Field Lab.
Students
Students are active students according to the block and semester they are taking. Students receive enrichment material regarding the content, technical aspects, and procedures for implementing the activity from the assigned field lab lecturer in coordination with the relevant block coordinator. Students bring equipment, consumables, and everything necessary when visiting the selected family/community group, such as students of KB/TK Aisyiyah, as instructed. Students receive guidance from the supervising lecturer regarding planning before going to the field, during the field work, and in preparing the activity report. Students submit the activity report after conducting observation, screening, and education to the fostered family or group in the field. The technical procedure for submitting the report is determined by the Head of the Field Lab in coordination with the relevant block coordinator.
Campus Supervising Lecturer
Campus supervising lecturers are FK UMS lecturers selected by the Head of the Field Lab in coordination with the Head of the Undergraduate Medical Study Program, taking into account the workload of the lecturers concerned. The supervising lecturers receive perception alignment guidance from the Head of the Field Lab regarding the Field Lab learning activities in the relevant block and semester. The campus supervising lecturers provide assistance related to the planning, implementation, and report preparation for their supervised student groups. This mentorship is expected to result in the most optimal learning experience and performance from their supervised student groups. The supervising lecturers may provide an assessment of the activity reports/performance of their supervised students if necessary.
Field Mentor
Field mentors are the posyandu cadre organizations / KB/TK (Kindergarten/Playgroup) teachers and supervisory midwives / KB/TK principals up to the Head of the Community Health Center (Puskesmas) as the main person in charge and coordinator in the field. Field mentors are obligated to provide assistance in the field so that students can gain learning experience and perform optimally in the execution of the related Field Lab practicum.
Head of the Field Lab
The Head of the Field Lab is a permanent lecturer who receives an official assignment decree (SK) regarding the implementation of Field Lab activities, ranging from planning, execution, assessment, to evaluation. The Head of the Field Lab coordinates with the head of the Undergraduate Medical Study Program in appointing campus supervising lecturers. The Head of the Field Lab coordinates with the block coordinator regarding the planning, execution, and assessment system for students’ Field Lab practical activities.
School and Fostered Village Locations
School and Fostered Village Locations

Lokasi TK Aisyiyah Tunggulsari – FK UMS

Lokasi TK Aisyiyah II Makamhaji – FK UMS

Lokasi TK Aisyiyah Karangasem Surakarta – FK UMS

Lokasi TK Aisyiyah Gonilan – FK UMS

Lokasi TK Aisyiyah Intan Permata Makamhaji – FK UMS

Lokasi Desa Binaan Kuwian, Banyudono - Boyolali

Lokasi Desa Binaan Mayang, Gatak - Sukoharjo
Field Lab Activities at Partner Schools

Field Activities with Fostered Villages